Topic B3 - Injury
A comprehensive study guide covering injury risk, classification, and management for IB SEHS 2026.
Mastering the key terminology of Topic B.3 is fundamental for demonstrating a precise and expert understanding in your IB SEHS exams. Accurate use of these terms allows you to articulate complex concepts with clarity, which is essential for scoring highly. The following list covers the essential vocabulary related to injury risk, classification, and management. It is crucial to understand these definitions before exploring how they are applied in the exam questions that follow.
Understanding these terms with precision is crucial, as they form the foundation for discussing injury mechanics, prevention strategies, and recovery protocols in your SEHS examinations.
Within this structure, questions are framed using specific "command terms" that dictate the type of response required.
Command terms are the directive verbs used in exam questions that define the required depth and scope of your response. A common error is to 'explain' when asked to 'outline', or 'describe' when asked to 'evaluate'. Mastering the precise meaning of each command term is therefore essential for accessing the full range of marks available for any given question. The following table provides the official IB definition for key command terms and a model question and answer specific to Topic B.3.
| Command Term | IB Definition | B.3 Model Question & Answer |
|---|---|---|
| State | Give a specific name, value or other brief answer without explanation or calculation. | Q: State two congenital risk factors for
injury. A: Two congenital risk factors are structural abnormalities that affect bones, joints, ligaments or muscles, such as joint hypermobility, and neurological conditions, such as cerebral palsy p.374. |
| Outline | Give a brief account or summary. | Q: Outline the graduated return to sport strategy
following a
concussion. A: The strategy consists of six stages: (1) symptom-limited activity, (2) light aerobic exercise, (3) sport-specific exercise without head impact, (4) non-contact training drills, (5) full contact practice following medical clearance, and finally (6) return to normal game play p.394. |
| Describe | Give a detailed account. | Q: Describe biomechanical maladaptation as a risk
for
injury. A: Biomechanical maladaptation refers to inefficient movement patterns that cause certain body parts to be subjected to excessive stress or load. For example, when a soccer player's knee collapses inward when kicking (knee valgus), it puts a lot of strain on the knee joint. By identifying and correcting these imbalances through exercises and coaching, an athlete can improve movement efficiency, reduce stress on vulnerable areas, and decrease the risk of sport-related injuries p.382-383. |
| Explain | Give a detailed account including reasons or causes. | Q: Explain how age can be an internal risk factor
for injury in
adolescent
athletes. A: During adolescence, athletes experience rapid growth spurts. This skeletal growth can create a size difference between the bone and soft tissue, as the soft tissue may not lengthen until the skeletal growth has slowed. This imbalance can increase the injury risk of, for example, ankle sprains. Furthermore, young athletes are at a higher fracture risk in specific areas of the long bone involving the junction between the epiphyseal plates and the formed bone, as these growth plates are weaker than articular cartilage p.371. |
| Analyse | Break down in order to bring out the essential elements or structure. | Q: Analyse the role of protective equipment in
preventing
musculoskeletal
injury. A: Protective equipment is a key external factor in reducing injury risk by preventing or mitigating the forces that cause trauma. For example, wrist guards used in snowboarding create a significant protective effect in reducing the risk of wrist fracture and wrist sprains p.375. Similarly, taping an ankle can reduce re-injury by over 71% by providing external support p.375. However, the effectiveness of equipment depends on proper use and fit; for example, in rugby, modern headgear is designed to reduce cuts and abrasions but offers almost zero injury prevention for concussions to the head region p.375. Therefore, while essential, equipment must be sport-specific and used correctly to be effective. |
| Evaluate | Make an appraisal by weighing up the strengths and limitations. | Q: Evaluate the use of the RICE protocol in the
initial
treatment of acute
musculoskeletal injuries. A: The RICE (Rest, Ice, Compression, Elevation) protocol is a widely known method for acute injury management. Strengths: 1. It is simple to remember and apply, making it accessible for initial first aid by athletes, coaches, and parents. 2. The components aim to reduce pain and swelling, which can provide immediate relief and comfort to the injured athlete p.392. Limitations: 1. There is scientific debate about whether applying ice and suppressing inflammation, a natural part of the healing process, could potentially delay recovery in the long term p.393. 2. The protocol has been updated by newer acronyms like POLICE (Protection, Optimal Loading, Ice, Compression, Elevation), which emphasize the importance of appropriate, early 'optimal loading' to stimulate healing, a crucial element missing from the simple 'rest' component of RICE p.392. |
| Calculate | Obtain a numerical answer showing the relevant stages in the working. | Q: In a study by Emery et al. (2020), the
intervention group of
655
students had 51 lower limb injuries. The control group of 501
students had 35
lower limb
injuries. Calculate which group had the lower injury incidence rate
per 1,000
students. A: Formula: Injury Rate = (Number of injuries / Number of participants) * 1000 Working: Intervention Group: (51 injuries / 655 participants) * 1000 = 77.86 injuries per 1,000 students. Control Group: (35 injuries / 501 participants) * 1000 = 69.86 injuries per 1,000 students. Answer: The control group had the lower incidence rate of lower limb injuries at 69.86 per 1,000 students (Data adapted from p.397). |
The following section provides the detailed content from which you can draw the knowledge required to construct such answers.
This section deconstructs the core content of Topic B.3, providing the essential knowledge required for the exam. It begins by examining the multifaceted causes of sports injuries, from individual predispositions to environmental hazards, before moving on to analyze the scientific interventions used to prevent, treat, and manage them.
B.3.1 Causes of Injury
Understanding the complex interaction of various risk factors is the first step toward effective injury prevention. This sub-topic explores the 'why' behind injuries, examining how different factors can predispose an athlete to harm. It covers the fundamental concepts of risk assessment and the classification of injuries, providing a framework for analyzing how and why injuries occur in sport and exercise.
Key Concepts:
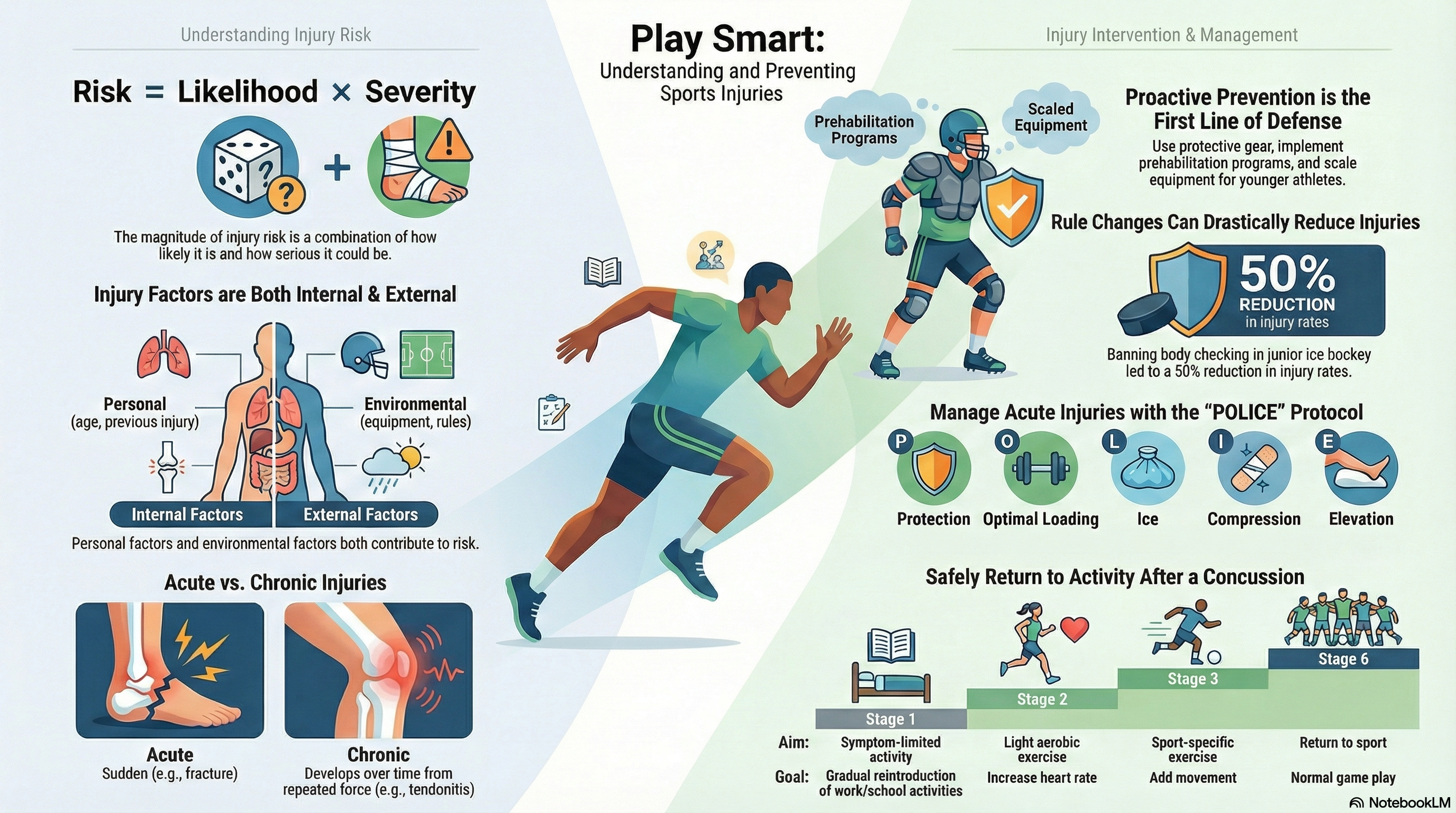
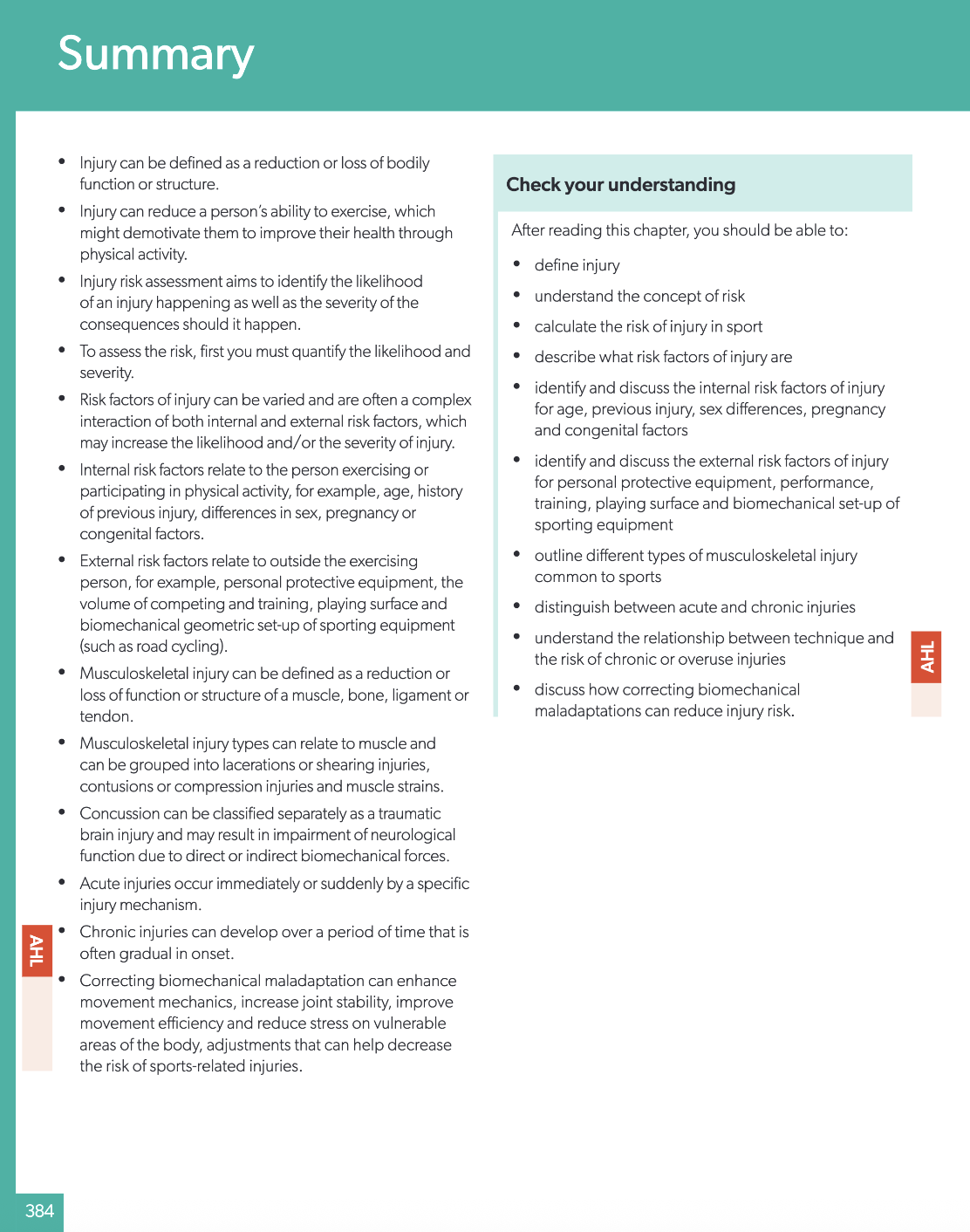
- Injury can be defined as a reduction or loss of bodily function or structure p.367.
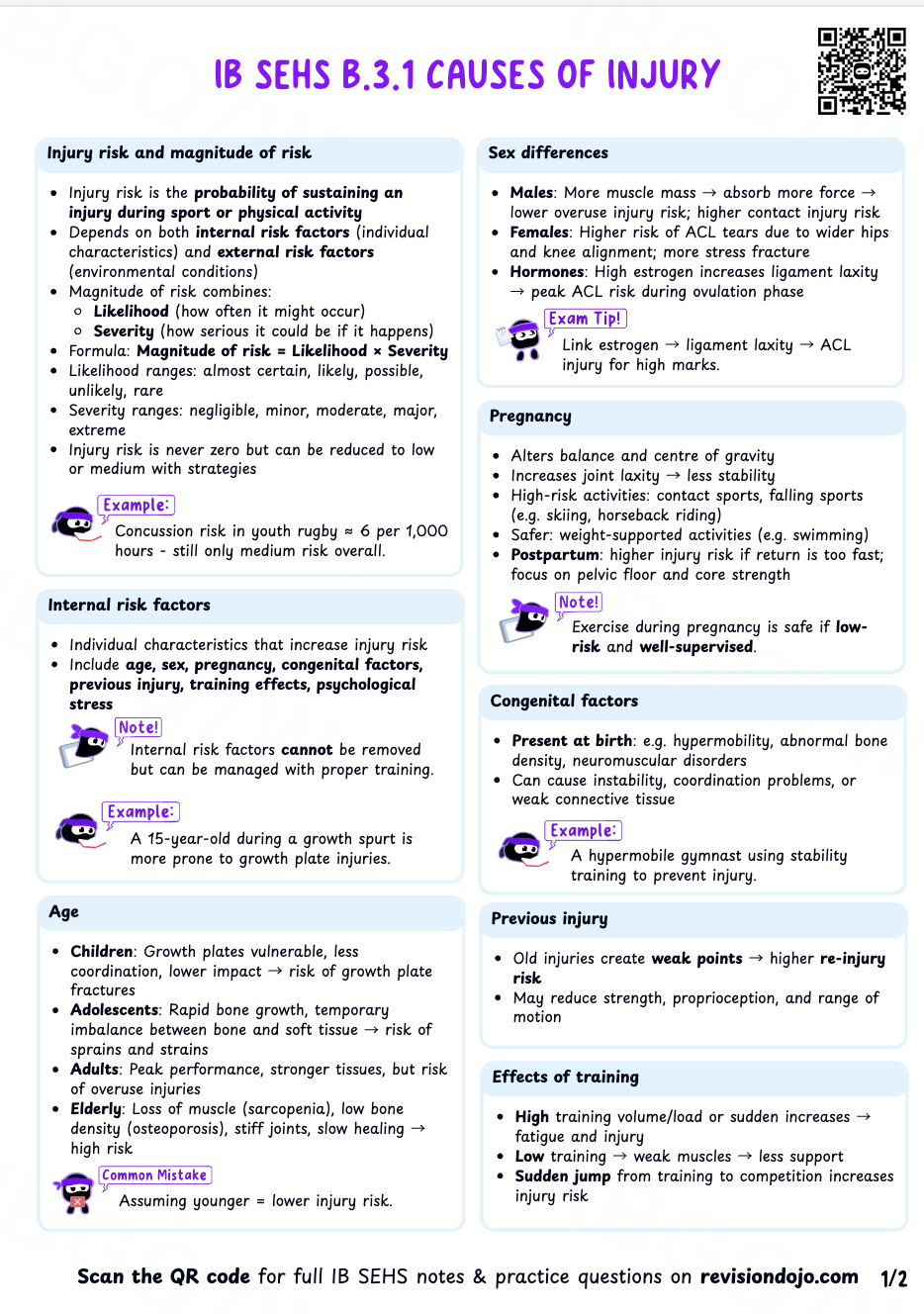
- Risk is a product of the likelihood of an injury occurring and its potential severity p.367.
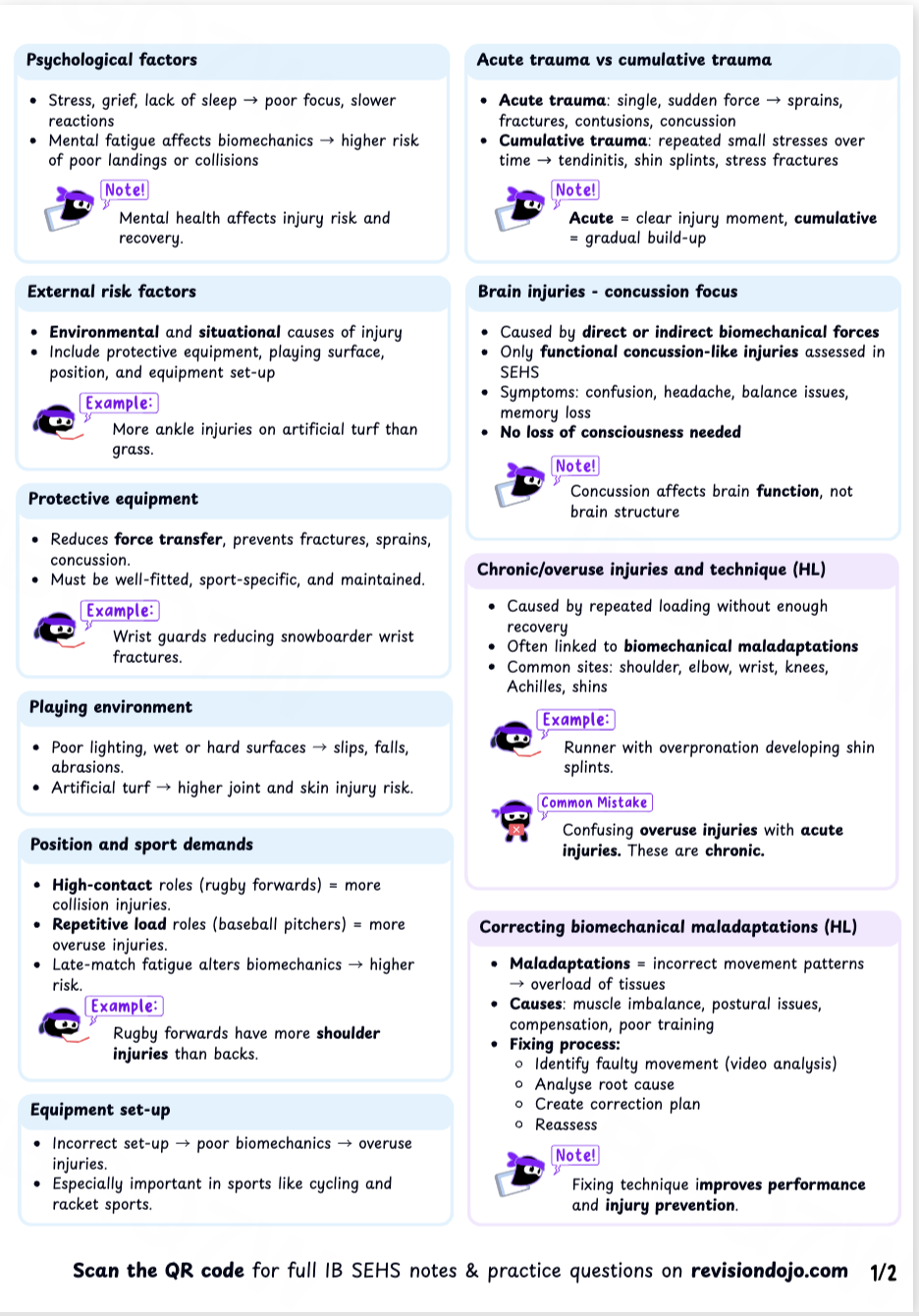
- Risk factors are categorized as internal (e.g., age, sex, previous injury) and external (e.g., equipment, playing surface) p.371.
- Injuries can be classified as acute (sudden onset) or chronic (overuse/gradual onset) p.380-381.
- Biomechanical maladaptation, or poor movement technique, can significantly increase stress on joints and tissues p.382.
Mechanism Explained: How Previous Injury Increases Future Injury Risk
- An athlete sustains an initial injury (e.g., an ankle sprain).
- Even after the pain subsides, rehabilitation may be incomplete, leading to a reduced range of movement, decreased strength, or impaired proprioception (the sense of body position) p.372.
- When the athlete returns to sport, these deficits alter their biomechanics, placing abnormal stress on the injured joint or compensatory stress on other body parts.
- This altered movement and lack of full recovery significantly increases the likelihood of re-injuring the same area or sustaining a new injury elsewhere p.372.
In youth rugby, the risk of injury from tackling increases due to the volume of training and competition. An adolescent player experiencing a growth spurt is particularly vulnerable to fractures at the epiphyseal plates (growth plates) because these areas are weaker during periods of rapid bone growth p.371.
For scientific analysis, injuries are often measured using "injury incidence rate," which standardizes the number of injuries per 1,000 hours of participation. This allows for fair comparisons between sports with different season lengths and squad sizes.
B.3.2 Interventions Related to Injury
Once the causes of injury are understood, targeted interventions can be designed and implemented to protect athletes. This sub-topic analyzes the proactive and reactive strategies used to reduce injury risk, manage injuries effectively when they occur, and facilitate a safe and timely return to activity. It covers everything from rule changes and equipment mandates to structured rehabilitation protocols.
Key Concepts:
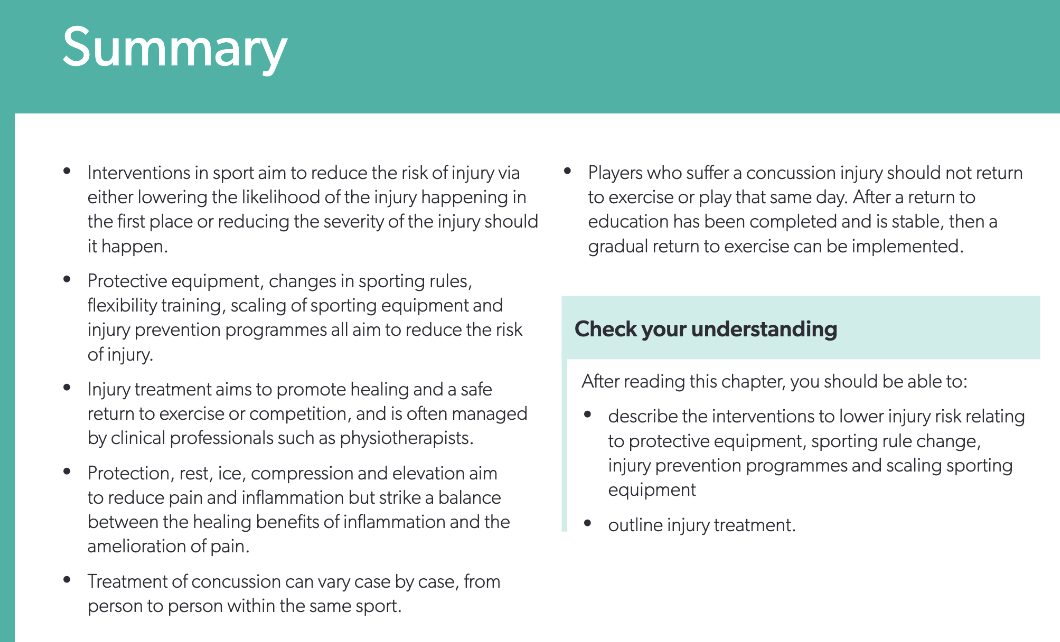
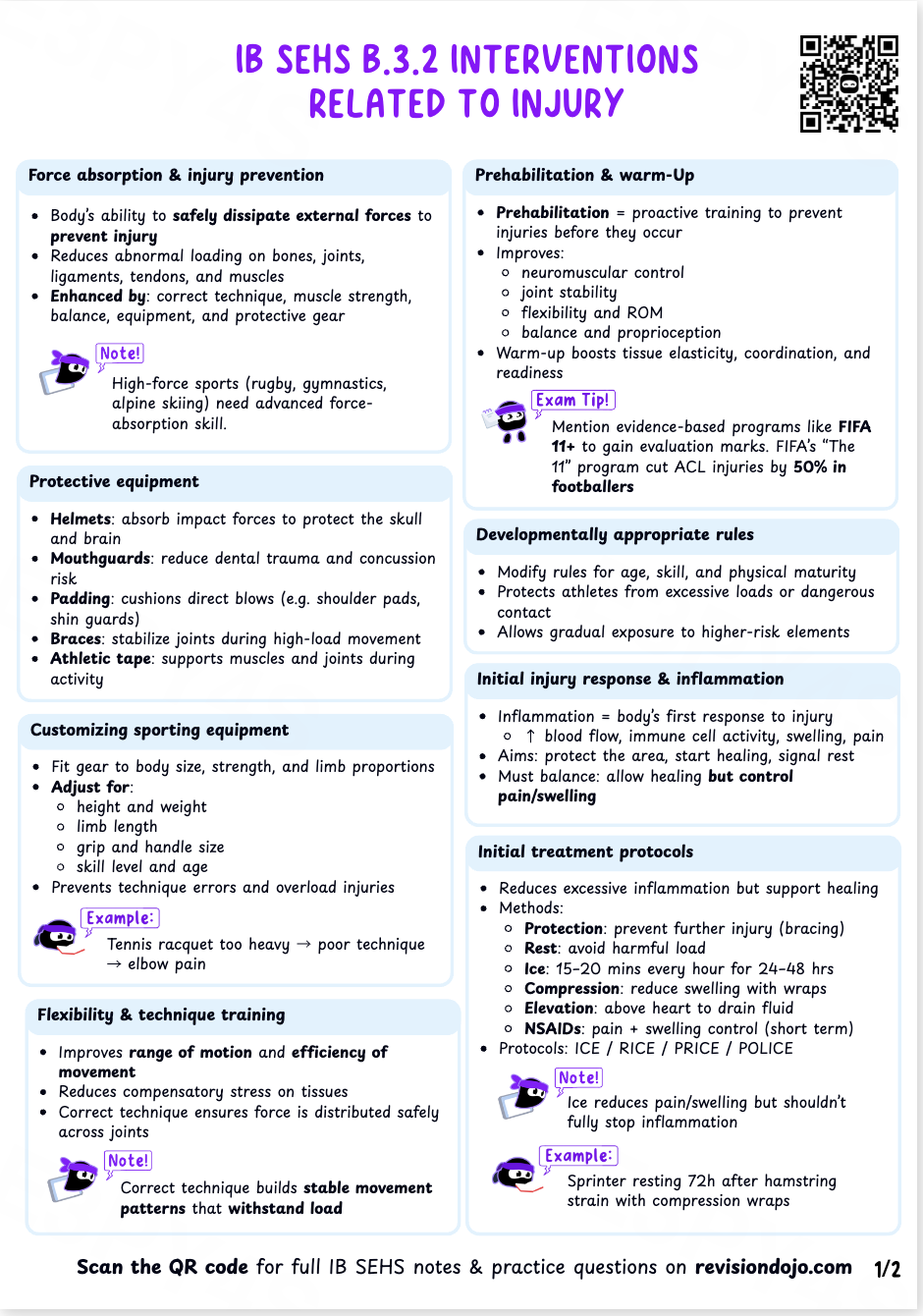
- Interventions aim to lower injury risk by reducing the likelihood of it happening or minimizing its severity p.386.
- Methods include modifying rules (e.g., banning certain tackles), mandating protective equipment, and implementing structured prehabilitation programmes p.387-388.
- Injury prevention programmes, like the FIFA 11+, combine neuromuscular training, balance, and strength exercises to reduce injury rates p.388-389.
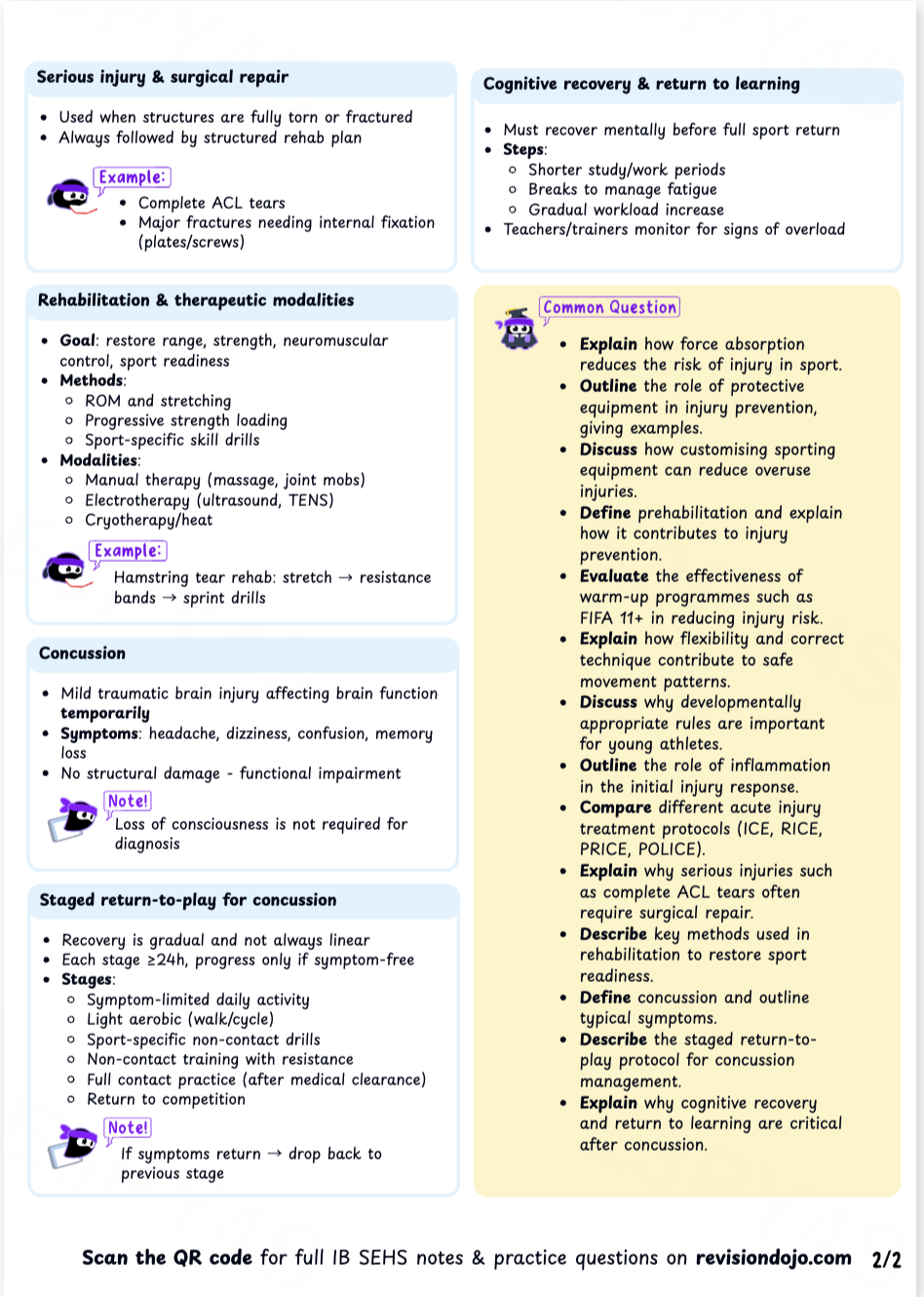
- Acute injury treatment has evolved from RICE to protocols like POLICE, which emphasizes optimal loading to promote healing p.392.
- Concussion management requires a strict, graduated return-to-play protocol to ensure the brain has fully recovered before exposing it to further risk p.394.
Mechanism Explained: How the POLICE Protocol Facilitates Healing
- Protection: The injured area is protected from further damage immediately after the injury.
- Optimal Loading: Instead of complete rest, gentle, pain-free movement is introduced early. This stimulates the tissue, promotes lymphatic drainage, and helps align new collagen fibres, leading to stronger, more functional scar tissue.
- Ice: Cryotherapy is applied to reduce pain (analgesia) and potentially limit secondary damage from inflammation p.392.
- Compression: An elastic bandage is used to reduce oedema (swelling) by increasing the pressure of the external tissue, which promotes lymphatic drainage p.392.
- Elevation: Raising the injured limb above the heart uses gravity to aid the return of fluid from the injured area p.392.
In soccer, the FIFA 11+ programme is a standardized warm-up used to reduce injuries. It includes running exercises, strength, plyometrics, and balance. Studies have shown it leads to a 21% reduction in total injury rates, and has been shown to be particularly effective for young female players, with some studies finding injury rate reductions of up to 50% p.389.
Be aware of the ongoing scientific debate about the use of ice (cryotherapy). While it reduces pain, some research suggests it might slow down the necessary inflammatory response needed for tissue repair. However, for the purpose of the exam, focus on its role in pain management and minimizing secondary hypoxic injury as per the textbook p.393.
Applying your knowledge through exam-style questions is a critical step in preparation. It helps to consolidate your understanding and develop the skills needed to construct clear, accurate, and well-supported answers under time pressure. This section provides a range of question types, from multiple-choice to data-based and extended response, to build your exam confidence and technique.
Why A is wrong: An ankle fracture from a tackle is caused by a sudden, excessive application of force, which is an acute injury p.380.
Why B is wrong: A concussion from a collision is a traumatic brain injury that occurs immediately, classifying it as an acute injury p.379.
Why D is wrong: A laceration is a cut that occurs from an immediate event, making it an acute injury p.378.
Why A is wrong: Bike geometry is an aspect of equipment set-up, which is an external risk factor p.377.
Why B is wrong: The playing surface is an environmental condition outside of the person, making it an external risk factor p.377.
Why D is wrong: Protective equipment is an external factor that an athlete uses p.375.
Why A, C, and D are wrong: These are incorrect terms. The protocol specifically uses the term Optimal Loading to replace the simple concept of 'Rest' from the older RICE protocol p.392.
Why A is wrong: While running exercises are part of the warm-up, the key components for neuromuscular control are balance and plyometrics.
Why B and D are wrong: Scaling equipment and rule changes are other types of injury interventions but are not components of the FIFA 11+ programme itself p.388, 390.
Why B is wrong: The 21% reduction figure is associated with the FIFA 11+ programme in soccer p.389.
Why C is wrong: Increasing the crash mat area was an intervention for pole vaulting p.388.
Why D is wrong: The 71% reduction refers to the effectiveness of ankle taping in preventing re-injury p.375.
The questions below provide insight into the types of challenges you will face in Paper 1B. Unlike standard knowledge checks, this component places a distinct emphasis on data analysis and experimental work.
Success in Paper 1B requires you to apply the "Nature of Science" (NOS) skills—such as evaluating methodologies, interpreting graphs, and understanding study design—rather than simply recalling course content.
To access a complete archive of true past papers and exemplar materials for Paper 1B, please use the resource link below.
| Injury type | n | % |
|---|---|---|
| abrasion | 316 | 64 |
| contusion | 279 | 57 |
| torsion | 72 | 15 |
| laceration | 62 | 13 |
| strained muscle | 45 | 9 |
| fracture | 33 | 7 |
| concussion | 23 | 5 |
| ligament strain | 23 | 5 |
| joint dislocation | 15 | 3 |
| joint inflammation | 7 | 1 |
| ligament rupture | 4 | 1 |
| others | 23 | 5 |
Identify the most common type of injury sustained by the mountain bikers. [1 mark]
Calculate the combined percentage of injuries that were either a fracture or a concussion. [1 mark]
Using the data and your own knowledge, explain why protective equipment such as helmets and pads is strongly recommended for downhill mountain biking. [3 marks]
| Sport and sex characteristic | Acute injuries (%) | Overuse injuries (%) | Total injuries |
|---|---|---|---|
| soccer, male | 90.62 | 9.38 | 4,042 |
| basketball, male | 93.61 | 6.39 | 4,179 |
| soccer, female | 90.79 | 9.21 | 4,988 |
| basketball, female | 90.70 | 9.30 | 4,065 |
Calculate the total number of overuse injuries recorded for female basketball players. [2 marks]
Compare the percentage of acute injuries between male and female soccer players. [1 mark]
Explain one reason why overuse injuries like tendonitis or shin splints may occur in a sport like basketball. [2 marks]
Identify the most common area for overuse injuries in Year 1. [1 mark]
Calculate the approximate percentage point difference for knee injuries between Year 1 and Year 5. [1 mark]
Explain two reasons why army recruits might be susceptible to overuse injuries in the lower limbs (knee, ankle/foot, calf/shin). [2 marks]
For the long-distance runner, the repetitive impact of each foot strike during many hours of training places continuous stress on the bones, tendons, and ligaments of the lower limbs. [1 mark] An example is shin splints (tendonitis), where the muscles and tendons surrounding the tibia become inflamed due to the repeated stress of running, especially with training errors like a sudden increase in mileage or intensity. [1 mark]
For the baseball pitcher, the biomechanics of the throwing motion involve extremely high velocities and forces at the shoulder and elbow joint. [1 mark] Repeating this motion hundreds of times a week leads to cumulative microtrauma to the soft tissues. This can result in an overuse injury like a rotator cuff strain or tendonitis. [1 mark]
In both cases, the injury is not from a single event but from an accumulation of stress that exceeds the body's ability to repair itself between training sessions, often due to factors like excessive training volume, biomechanical maladaptation, or insufficient recovery. [1 mark]
Stage 1: Symptom-limited activity. The goal is cognitive and physical rest. The athlete performs daily activities that do not provoke symptoms. [1 mark]
Stage 2: Light aerobic exercise. The goal is to gradually increase heart rate. This involves activities like walking or stationary cycling at a slow to medium pace. [1 mark]
Stage 3: Sport-specific exercise. The goal is to add movement. The athlete can begin activities like skating drills, but with no head impact activities. [1 mark]
Stage 4: Non-contact training drills. The goal is to increase exercise, coordination, and cognitive load. The athlete can participate in more complex drills like passing, but still avoids physical contact. [1 mark]
Stage 5: Full contact practice. The goal is to restore confidence and assess functional skills. Following medical clearance, the athlete can participate in normal training activities to ensure they are ready for the physical demands of the game. [1 mark]
The final stage is Stage 6: Return to sport, where the athlete is cleared for normal game play. (Information synthesized from the table on p.394).
While SEHS is not a math-heavy subject, the ability to perform basic calculations and correctly interpret quantitative data related to injury is a key scientific skill. This section focuses on the primary calculation you will encounter in this topic.
Calculating Injury Incidence Rate
This calculation allows for a standardized comparison of injury risk between different groups or over time.
(The most common standardized time unit is per 1,000 hours of participation.)
Worked Example:
A study on youth rugby finds that in a season with a total of 2,000 hours of player participation (all players' hours combined), there were 50 reported concussions. Calculate the injury incidence rate per 1,000 hours.
Step 1: Identify the variables
- Total number of injuries = 50
- Total exposure time = 2,000 hours
- Standardized time unit = 1,000 hours
Step 2: Apply the formula
- Incidence Rate = (50 / 2,000) * 1,000
Step 3: Calculate the result
- Incidence Rate = 0.025 * 1,000
- Incidence Rate = 25
Conclusion
The injury incidence rate is 25 concussions per 1,000 hours of play. (Concept from p.370).
Understanding these calculations is important, but it is equally important to avoid common content-related errors.
Awareness of common misconceptions and exam errors is a powerful tool for revision. By understanding the pitfalls other students fall into, you can proactively avoid them and secure valuable marks. This section highlights content-specific errors related to Topic B.3.
A key skill for high achievement in IB SEHS is the ability to connect ideas across different topics.
IB SEHS rewards students who can synthesize information and make meaningful connections across different areas of the syllabus. High-level responses often demonstrate how concepts from one topic influence or interact with concepts from another. The following prompts are designed to help you practice this synoptic thinking, integrating your knowledge of B.3 with other key topics.
- Consider the risk of injury from overloading (training too much, too soon) leading to overuse injuries.
- Consider the risk of injury from underloading (being unprepared for the demands of competition).
- Think about how progressive overload allows for physiological adaptations like increased collagen production in tendons, making them more resilient to injury.
- Relate training errors in volume, duration, or intensity to the development of both acute and chronic trauma.
- Recall that biomechanical maladaptation (e.g., knee valgus) is a risk factor for injury.
- Consider how a coach could modify task constraints (e.g., asking an athlete to land softly from a jump) or environmental constraints (e.g., using unstable surfaces for balance) to encourage the athlete to self-organize and discover a more efficient and safer movement pattern.
- Think about how this approach uses problem-solving rather than direct instruction to correct faulty mechanics.
- Connect mental toughness to an athlete's resilience and ability to handle the setbacks and emotional challenges of a long rehabilitation process.
- Consider how a positive mindset and high motivation can improve adherence to demanding and often painful rehabilitation exercises.
- Relate mental toughness to coping with pain and managing the stress associated with being unable to compete ('athletic identity').
Finally, use the checklist below to assess your overall readiness and identify any areas that require further review.
Use this checklist as a final, active revision tool to confirm your mastery of the key concepts and skills in Topic B.3 before an exam. Actively try to answer each question aloud or by writing a short summary. This will help you to honestly assess your confidence and pinpoint any remaining gaps in your knowledge.
- Can I define risk of injury and explain its two core components: likelihood and severity?
- Can I identify and describe at least three internal and three external risk factors for injury, providing a specific sporting example for each?
- Can I distinguish between an acute injury and a chronic injury, explaining the mechanism of each?
- Can I describe the characteristics of a contusion, a strain, and a concussion?
- Can I evaluate the effectiveness of three different interventions used to lower injury risk (e.g., protective equipment, rule changes, prehabilitation)?
- Can I outline the graduated return-to-play protocol that must be followed after a concussion?
- Can I explain the components of the POLICE protocol and justify why 'Optimal Loading' is a critical element?
- Can I calculate and interpret an injury incidence rate from a given data set?
🎉 Topic B3 - Injury Mastered!
You've completed the comprehensive study guide for injury in IB SEHS. Keep practicing with past papers and revisiting key concepts to maintain your expertise!